
Table of Contents >> Show >> Hide
- What exactly is dengue fever?
- Symptoms of dengue: what it feels like (and when)
- Severe dengue: warning signs you shouldn’t ignore
- Complications of dengue fever
- How dengue is diagnosed
- Dengue vs. look-alikes: why clinicians don’t guess
- What to expect if dengue is suspected
- Prevention (brief but practical)
- Experiences with dengue: what patients (and clinicians) say it’s really like
Dengue fever is one of those illnesses that can feel like “the worst flu you’ve ever had” (and then it has the audacity to come with a rash).
It’s caused by dengue viruses spread by Aedes mosquitoestiny insects with big opinions about personal space.
Most people recover with supportive care, but dengue can sometimes turn serious fast, especially around the time the fever breaks.
This guide walks through the symptoms, the complications to watch for, and how clinicians diagnose dengueso you understand what’s happening and why timing matters.
What exactly is dengue fever?
Dengue is a mosquito-borne viral infection caused by four closely related dengue virus types (often called “serotypes”).
You can get dengue more than once, and a second infection with a different serotype can raise the risk of severe disease.
Dengue is common in many tropical and subtropical regions, and in the U.S. most cases are linked to travelthough limited local spread has been reported in some states and U.S. territories.
How it spreads (and why it’s not “just a travel bug”)
Dengue spreads when a mosquito bites someone who has dengue virus in their blood and later bites another person.
It doesn’t usually spread directly person-to-person the way a cold does. The big risk factors are mosquito exposure and being in (or traveling to) areas with dengue activity.
Because the mosquitoes that can transmit dengue exist in parts of the United States, public health agencies pay close attention to travel-related cases and occasional local transmission.
Symptoms of dengue: what it feels like (and when)
Dengue symptoms often start suddenly after an incubation period (the time between the bite and feeling sick).
A classic dengue pattern is: a high fever plus intense body aches, headaches, and sometimes a rash. It can be mistaken for influenza, COVID, malaria, or other infectionsespecially early on.
Common early symptoms
- High fever (often abrupt onset)
- Severe headache
- Pain behind the eyes (retro-orbital painfancy term, very un-fancy feeling)
- Muscle, joint, and bone pain (“breakbone fever” is a dramatic nickname, but people don’t invent that for fun)
- Nausea and vomiting
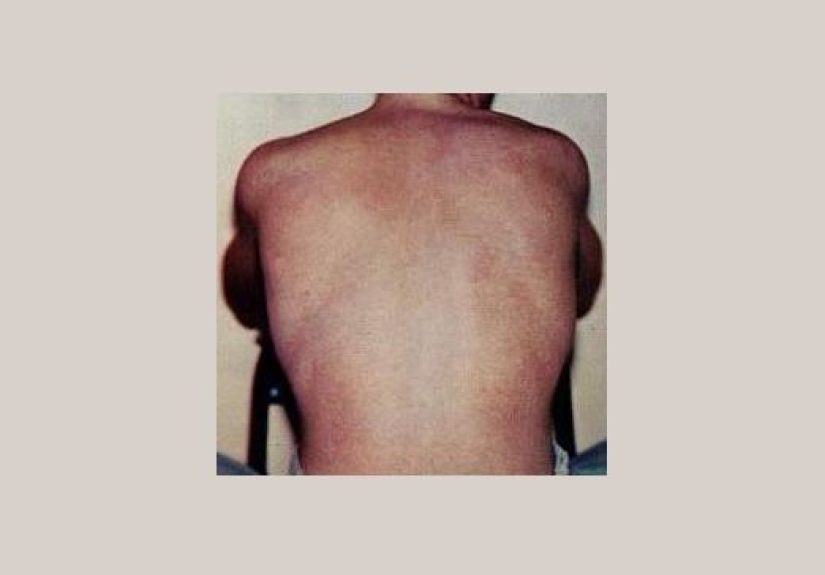
- Rash (often appears a few days into illness)
- Fatigue and a general “hit-by-a-truck” feeling
A helpful timeline: the “phases” clinicians think about
While every person is different, dengue is often described in phases because symptoms and risks can shift over time:
-
Febrile phase (early illness):
Fever and the classic pain symptoms dominate. Dehydration can become an issue if you’re sweating, not eating, or vomiting. -
Critical phase (often around when fever goes down):
This is the “pay attention” window. Some people begin improvingothers develop warning signs and can worsen quickly. -
Recovery phase:
Symptoms gradually improve, appetite returns, and energy starts to come back (though fatigue can linger).
Severe dengue: warning signs you shouldn’t ignore
Most symptomatic people recover, but dengue can sometimes progress to severe disease.
The tricky part is that severe dengue may begin after the fever starts to drop, when people think the worst is over.
This is why clinicians emphasize warning signs and close monitoring in higher-risk cases.
Warning signs (often after the fever breaks)
- Severe belly pain or tenderness
- Persistent vomiting (especially repeated vomiting in a day)
- Bleeding (such as nose or gum bleeding)
- Blood in vomit or stool
- Feeling extremely tired, restless, or unusually irritable
- Signs of fluid buildup (clinicians may look for this on exam or imaging)
What makes dengue “severe”?
Severe dengue is associated with problems such as significant plasma leakage (fluid shifting out of blood vessels), severe bleeding, shock, and organ impairment.
In real-world terms: the body’s circulation can become unstable, and that can become life-threatening without prompt medical care.
Not everyone with dengue warning signs develops severe dengue, but warning signs raise the urgency for evaluation and monitoring.
Complications of dengue fever
Dengue complications range from “I’m dehydrated and miserable” to severe illness requiring hospital-level support.
Complications are more likely in people with severe dengue, and in certain higher-risk groups.
1) Dehydration and electrolyte problems
High fever plus poor intake and vomiting can lead to dehydration.
Clinicians take this seriously because dehydration can worsen dizziness, weakness, and overall recoveryand may complicate the evaluation if lab values shift with fluid status.
2) Low platelets and bleeding risk
A hallmark lab finding in dengue is a drop in platelets (cells that help blood clot). This doesn’t automatically mean “you will bleed,”
but it helps clinicians assess severity and riskespecially when combined with other warning signs or evidence of plasma leakage.
3) Plasma leakage, shock, and breathing problems
In severe dengue, fluid can leak from blood vessels into surrounding tissues. That can reduce effective blood volume and contribute to shock.
Depending on where fluid collects, it may also contribute to breathing difficulty. This is one reason monitoringsometimes in a hospitalis recommended for people with warning signs.
4) Organ involvement (less common, but important)
Severe dengue can involve organs such as the liver, and in rare cases can affect the heart or nervous system.
Clinicians may check liver enzymes and other markers if symptoms suggest complications.
5) Pregnancy-related complications
Dengue during pregnancy is treated with extra caution. Studies and clinical guidance note risks such as preterm birth and low birth weight,
and clinicians also consider how dengue symptoms and lab changes could overlap with other pregnancy-related conditions.
How dengue is diagnosed
Dengue diagnosis is a combination of detective work and targeted lab testing.
Because symptoms overlap with many other illnesses, clinicians rely on exposure history (travel or residence in risk areas), timing of symptoms, exam findings,
and specific tests that detect dengue virus or the immune response to it.
Step 1: The history that matters (yes, travel counts)
Expect questions like:
- Where have you been in the last 2–3 weeks?
- Any mosquito exposure? Outdoor evening time? No screens? Lots of bites?
- When did the fever start (exact day)?
- Any warning signs since the fever began to drop?
Timing is crucial because the “best” diagnostic test depends on how many days it’s been since symptoms started.
Step 2: Physical exam clues
A clinician may look for dehydration, rash patterns, abdominal tenderness, and signs of bleeding.
They may also assess blood pressure trends, heart rate, and overall appearancebecause severe dengue can evolve quickly.
Step 3: Basic labs that support the picture
Even before confirmatory tests return, clinicians often order baseline labs to assess severity and complications:
- Complete blood count (CBC): may show low platelets and changes in white blood cells
- Hematocrit: can help assess hemoconcentration, which may suggest plasma leakage
- Liver enzymes: may be checked if there’s concern for liver involvement
Step 4: Confirmatory dengue testing (timing is everything)
The most commonly used approaches include:
- NAAT (such as RT-PCR): detects viral genetic material, typically most useful early in illness.
- NS1 antigen testing: detects a viral protein, typically used in the first week of symptoms.
- IgM antibody testing: detects an immune response that becomes more useful as days pass.
- IgG testing: can help interpret past vs. more recent infection patterns, depending on context.
Clinicians commonly pair an early viral test (NAAT or NS1) with antibody testing (IgM) to improve accuracy across the timeline.
If initial testing is negative but suspicion remains high, repeat testing may be consideredespecially for antibody-based results that can evolve over time.
Why false negatives and “confusing” results happen
Dengue testing isn’t confusing because labs are lazy; it’s confusing because biology is a chaotic artist.
Early in illness, the virus or NS1 antigen is more detectable. Later, the immune response becomes more detectable.
Testing too early or too late with the wrong test can miss infection.
Antibody tests can also cross-react with other related viruses in the same family, depending on exposure and vaccination history.
Dengue vs. look-alikes: why clinicians don’t guess
Dengue can resemble other infections that also require prompt diagnosis and treatment decisions.
Depending on travel history and symptoms, clinicians may evaluate for conditions like malaria (which can be life-threatening),
chikungunya, Zika, typhoid fever, leptospirosis, viral hepatitis, and more.
The goal is not to collect diagnoses like trading cardsit’s to identify what needs immediate action.
A quick example (how diagnosis often plays out)
Imagine a traveler returns from a dengue-risk region and develops sudden high fever, headache, and intense body aches on day 5 after coming home.
In the clinic, the clinician asks about travel dates and symptom onset, orders a CBC (to check platelets), and sends dengue testing that includes a viral detection test (like NAAT)
plus an IgM antibody test. If the patient later develops severe abdominal pain or persistent vomiting after the fever drops, they’re instructed to seek urgent care for reassessment and monitoring.
What to expect if dengue is suspected
Because there’s no single antiviral that cures dengue, care focuses on monitoring and supportive treatmentespecially hydration and watching for warning signs.
Clinicians may recommend follow-up labs, return precautions, or hospital evaluation depending on risk, symptoms, and lab trends.
Medication caution (a common clinical reminder)
Clinicians often advise avoiding certain pain relievers that may increase bleeding risk in suspected dengue.
If you’re ill and dengue is on the table, it’s worth asking your clinician what’s safest for fever and pain.
Prevention (brief but practical)
Since dengue is mosquito-borne, prevention is mostly about bite avoidance: using EPA-registered insect repellent, wearing long sleeves when possible,
and reducing mosquito exposure (screens, air conditioning, eliminating standing water).
In the U.S., dengue vaccination recommendations are limited and targeted to specific pediatric groups in dengue-endemic areas with confirmed prior infection.
Experiences with dengue: what patients (and clinicians) say it’s really like
The clinical descriptions of dengue are accuratebut they can feel oddly sterile compared to how the illness lands in real life.
When people talk about dengue, they rarely start with “I had a febrile illness.” They start with: “I felt fine at breakfast and wrecked by lunch.”
That sudden onset is a recurring theme. Many patients describe a fast-rising fever and a deep, all-over ache that makes it hard to sleep, sit still, or even scroll on a phone without wincing.
It’s not just pain; it’s the combination of fever, headache, and total-body heaviness that makes normal tasks feel like a marathon in wet jeans.
Another common experience is confusion in the first couple of daysbecause dengue can look like so many other infections.
Travelers often assume it’s jet lag, a stomach bug, or “something I ate.” Parents sometimes think it’s influenza.
People who live in areas with lots of mosquito bites may not connect the dots right away because, honestly, who keeps a diary of every bite?
In clinics, one of the most useful moments is when someone remembers a key detail: “I just got back from a trip,” or “My neighbor mentioned dengue cases,” or “Everyone on the excursion got eaten alive.”
That’s usually when the clinician’s questions become more specific, and testing decisions get sharper.
People are often surprised by how much the timing matters. Some patients get tested very early, see an initial negative result,
and assume they’re in the clearonly to learn that certain tests work best at particular points in the illness.
Clinicians see this a lot, which is why they sometimes pair tests (like a viral detection test plus an antibody test) and, if needed, repeat testing later.
From the patient perspective, it can feel like, “So… do I have dengue or not?” From the clinician perspective, it’s more like,
“Let’s match the right tool to the right day of illness so we don’t miss what’s in front of us.”
The fever-breaking moment is another story people remember. Many patients expect that once the fever drops, they’re automatically better.
Sometimes that’s trueand the next few days are about resting, rehydrating, and gradually feeling human again.
But some people describe a more unsettling turn: new stomach pain, repeated vomiting, dizziness, or an abrupt sense that something is “off.”
Clinicians emphasize these warning signs because severe dengue can begin around this time, and early evaluation can make a major difference.
Patients who sought care quickly often describe a clear plan: observation, repeat labs, careful hydration, and close monitoring for changes.
Not dramatic heroicsjust steady, careful medical attention.
Recovery stories also have a pattern: the fever and worst pain may resolve within about a week, but the fatigue can hang around longer than expected.
People describe feeling “out of battery” for days or weeksneeding naps, losing stamina, and struggling to bounce back to normal workouts or busy schedules.
This can be frustrating, especially for people who are otherwise healthy and active. Clinicians often reassure patients that gradual recovery is common,
and they focus on hydration, nutrition, and pacingbecause trying to “power through” too soon can backfire.
If there’s one “wish I knew this earlier” takeaway from many dengue experiences, it’s this:
dengue is not just about the fever. It’s about the patternthe sudden onset, the classic pain symptoms, the possibility of a rash,
and the importance of watching for warning signs after the fever drops. The best outcomes tend to come from the same not-so-glamorous combo:
recognizing risk (especially travel or local alerts), getting evaluated at the right time, using the right tests for the right day of illness,
and taking warning signs seriously rather than hoping they’ll magically vanish because you drank a sports drink and said, “I’m fine.”






