
Table of Contents >> Show >> Hide
- What the knee jerk reflex actually tests (in plain English)
- Before you start: safety, comfort, and what you’ll need
- The knee jerk reflex test: 7 simple steps
- Step 1: Position the leg so it can swing freely
- Step 2: Ask for “floppy” relaxation (yes, really)
- Step 3: Find the targetthe patellar tendon, not the kneecap
- Step 4: Hold the reflex hammer the right way (wrist snap, not elbow smash)
- Step 5: Tap the tendon with a quick, controlled strike
- Step 6: Compare both sides, then try a reinforcement trick if needed
- Step 7: Grade what you saw and write down a simple note
- How to interpret results without panicking (or self-diagnosing)
- Common mistakes (so you don’t blame the nervous system for user error)
- When to stop DIY testing and call a professional
- Mini FAQ (because everyone asks these)
- Conclusion
- Real-world experiences: what it’s like to learn (and actually use) the knee jerk reflex test
The “knee jerk” reflex (also called the patellar tendon reflex) is the classic party trick of the medical world:
a quick tap below your kneecap andif your nervous system feels like cooperatingyour lower leg kicks out like it’s saying,
“I didn’t consent to this audition.”
In real life, this isn’t a parlor trick. It’s a basic piece of a neurological exam used to see how well a specific
reflex pathway is working. You can learn to check it at home for educational purposes, but this test does not diagnose anything by itself.
If you’re worried about symptoms (numbness, weakness, falls, severe back pain, new bladder issues, etc.), treat this as a “clue,” not a conclusion.
What the knee jerk reflex actually tests (in plain English)
When the tendon just below your kneecap is tapped, it briefly stretches the quadriceps muscle. Your body responds automatically by tightening that
muscle, which makes your leg extend a bit. That loop is a fast “wire → switchboard → wire” circuit involving sensory nerves, the spinal cord, and
motor nerves.
Clinicians often associate the patellar reflex mostly with the femoral nerve and spinal nerve roots around
L2–L4 (often emphasized as L4). That’s why it’s used as one small data point when checking for nerve irritation or other neurologic issues.
Also important: reflex strength varies a lot among healthy people, so the most helpful trick is comparing left vs. right.
Before you start: safety, comfort, and what you’ll need
What you’ll need
- A reflex hammer (best option). If you don’t have one, skip the DIY “hardware store” substitutesthis is not the moment for a claw hammer.
- A chair, bench, or bed where the person being tested can sit safely.
- Good lighting so you can see the kneecap area clearly.
- Optional: a phone note to record what you observed (not a full medical chartjust “left brisk, right normal,” etc.).
When NOT to test
- Recent knee surgery, a fresh knee injury, severe pain, significant swelling, or suspected fracture.
- If tapping causes sharp pain (discomfort is different from painpain is your stop sign).
- If the person has a condition where sudden leg movement could cause a fall and you can’t position them safely.
If you’re testing someone else, make sure they’re seated securely and can’t slide off the edge. Reflexes can surprise peopleespecially if they
“swear it won’t work” and then their leg pops out like it’s proving a point.
The knee jerk reflex test: 7 simple steps
Step 1: Position the leg so it can swing freely
The easiest setup is seated: have the person sit on a high chair or exam table so their lower legs dangle and the knees are bent around 90 degrees.
The goal is a relaxed, hanging lower legnot a leg braced against the floor like it’s preparing for a deadlift.
Alternative (if dangling isn’t possible): the person can lie on their back with the knee slightly bent and supported, but the seated/dangling method is
usually simpler for beginners.
Step 2: Ask for “floppy” relaxation (yes, really)
This test fails most often because the person is accidentally tensing their thigh. Tell them:
“Let your leg be heavy. Don’t help me. Don’t fight me. Just let it hang.”
A relaxed quadriceps muscle makes the reflex easier to see.
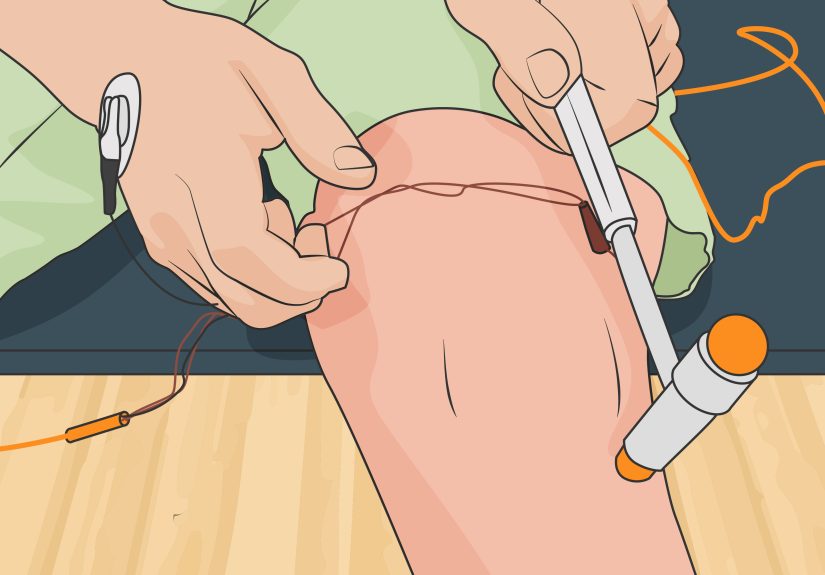
Step 3: Find the targetthe patellar tendon, not the kneecap
Place two fingers on the bottom edge of the kneecap (patella). Slide your fingers just below it. You’ll feel a firm band:
that’s the patellar tendon. This is what you tapnot the kneecap itself and not the shin.
If you’re unsure, ask the person to gently straighten their knee once, then relax again. The tendon may stand out briefly, making it easier to locate.
Step 4: Hold the reflex hammer the right way (wrist snap, not elbow smash)
Grip the hammer loosely near the end of the handle so it can swing. The motion should come mostly from the wrist, like you’re flicking water off your hand.
You’re aiming for a quick, elastic tapnot a slow push and definitely not a “let me wind up like a baseball pitcher.”
Step 5: Tap the tendon with a quick, controlled strike
Tap the patellar tendon briskly. Watch the lower leg and feel the quadriceps if needed (you can lightly place your other hand on the thigh).
A typical response is a brief knee extensionthe lower leg swings forward.
If nothing happens, don’t immediately assume something is “wrong.” First, troubleshoot technique: Was the tendon actually tapped? Was the leg relaxed?
Was the tap quick enough?
Step 6: Compare both sides, then try a reinforcement trick if needed
Repeat on the other knee and compare. In many real-world exams, side-to-side difference matters more than the absolute “strength” of a single reflex.
If reflexes seem hard to bring out, try the classic Jendrassik maneuver (a distraction/reinforcement technique):
have the person interlock their fingers and pull their hands apart firmly right as you tap the tendon. This can reduce “I’m accidentally tensing”
interference and make a subtle reflex easier to see.
Step 7: Grade what you saw and write down a simple note
Clinicians often use a rough grading scale. You don’t need to be fancy, but a simple structure helps:
- 0 = no response
- 1+ = small/diminished
- 2+ = “typical”/expected
- 3+ = brisk
- 4+ = very brisk; may include rhythmic “extra beats” (clonus)
Your note can be as simple as: “Left 2+, right 2+” or “Left brisk, right normal.” If you used reinforcement, note that too:
“Right 1+ without, 2+ with Jendrassik.”
How to interpret results without panicking (or self-diagnosing)
Reflexes are influenced by lots of normal factors: how relaxed you are, whether you’re cold, anxious, distracted, or even how skilled the tester is.
One “weird” result in a living-room test is not a medical verdict.
What “reduced” reflexes can suggest
A reduced or absent patellar reflex can occur if the reflex pathway is disrupted somewhere along the chainperipheral nerve issues, nerve root problems,
or muscle/neuromuscular conditions. It can also show up in perfectly healthy people, especially if they’re tense or the tap missed the tendon.
That’s why clinicians look for a pattern across multiple findings (strength, sensation, gait, other reflexes), not one tap.
What “brisk” reflexes can suggest
A very brisk reflex, especially if paired with clonus (repeated rhythmic beats), can be a sign of increased reflex activity that clinicians sometimes see
with certain central nervous system conditions. But again: context matters, and “brisk” can also be a normal variant.
Common mistakes (so you don’t blame the nervous system for user error)
- Tapping the kneecap instead of the tendon below it.
- Leg braced on the floor so it can’t swing and you can’t see movement.
- Slow pushing instead of a quick tap (reflexes like “boing,” not “shove”).
- Tester overthinking and under-tappingcontrolled, not timid.
- Person being tested tensing up because they’re anticipating the hit (use relaxation cues or Jendrassik).
- Not comparing sides (you lose one of the most useful reference points).
When to stop DIY testing and call a professional
If you have concerning symptoms, don’t try to “reflex your way” into an answer. Contact a clinician promptly if you notice:
- New or worsening weakness, trouble walking, frequent tripping, or falls
- Numbness/tingling that’s spreading or persistent
- Severe back pain with leg weakness or sensory changes
- Major left-right differences that are new and you also have symptoms
- Any bowel/bladder changes with leg symptoms (urgent evaluation)
Think of the knee jerk reflex as one dashboard light. Useful? Yes. The whole car diagnostic? No.
Mini FAQ (because everyone asks these)
Does it mean something is wrong if my leg barely moves?
Not necessarily. Many healthy people have subtle reflexes, and technique matters a lot. Make sure the leg is relaxed and free-hanging, strike the tendon
(not the kneecap), compare both sides, and try reinforcement before drawing any conclusions.
Can I test this without a reflex hammer?
You can learn the concept, but for a reliable, safe tap, a reflex hammer is the right tool. Improvised hard objects increase the risk of pain or injury
and don’t improve accuracy.
Why do doctors care about reflexes at all?
Reflexes offer quick information about how nerves, spinal cord connections, and motor pathways are functioning. They’re fast, inexpensive, and can help
guide a broader examespecially when paired with strength and sensation testing.
Conclusion
Testing the knee jerk reflex is simple once you know the basics: a relaxed leg, the correct tendon landmark, a quick wrist-driven tap, and side-to-side
comparison. Add the Jendrassik maneuver when you’re not seeing much, and remember that interpretation depends on the full picturenot a single “kick.”
If you’re testing because you’re worried about symptoms, let this be a starting point for a real medical evaluation, not a substitute for one.
Real-world experiences: what it’s like to learn (and actually use) the knee jerk reflex test
If you’ve never tested a knee jerk reflex before, your first experience is usually one of two extremes: either “Nothing happened and now I feel awkward,”
or “Wow, that leg just launched like it had places to be.” Both are normal beginner momentsand they teach the same lesson: technique and relaxation matter
more than drama.
A common learning experience is discovering how much people tense up without realizing it. The person being tested often says, “I’m relaxed,” while their
quadriceps is clenched like it’s guarding national secrets. When you ask them to let the leg hang heavy, you’ll sometimes see the whole posture change:
shoulders drop, jaw unclenches, and suddenly the reflex shows up. This is why clinicians talk so much about patient comfort. It’s not bedside manners for
its own sake; it literally changes the exam.
Another classic experience happens when someone tries to “help” the test. They might subtly straighten their knee right as you tapalmost like they want
to prove they’re functioning. The funny part is that this makes the reflex harder to interpret, because now you’re watching a voluntary movement mixed with
a reflex movement. In teaching settings, instructors will often say something like, “Don’t let them assistreflexes are a surprise party, not a scheduled
meeting.” The more you practice, the easier it becomes to spot the difference between a reflex kick (brief, automatic) and a deliberate extension (slower,
more controlled).
Many learners also have a “lightbulb moment” with the Jendrassik maneuver. At first it seems weirdwhy would pulling your hands apart affect your knee?
Then you try it and realize how often the problem isn’t the nerves, it’s attention and muscle tension. People who are anxious, ticklish, or trying too hard
to stay still can accidentally dampen their reflex. Giving the brain another job (like hand pulling) often reduces that interference. When the reflex suddenly
appears, it feels less like magic and more like your first real understanding that the nervous system is always negotiating with the mind.
In everyday life, people often become interested in this test after a doctor checks their reflexes and they wonder what it meant. Some report being surprised
by how gentle a proper reflex hammer tap should bemore “quick bounce” than “hit.” Others notice that their reflex changes depending on how tired they are,
whether they’ve been sitting cross-legged, or how cold the room is. While home testing can’t confirm causes, these observations do mirror a reality of exams:
reflex responses can vary with the testing conditions, which is why clinicians compare sides, repeat taps, and look for patterns.
One of the most useful experiences you can gain is learning to document what you actually saw, not what you think it “should” mean. Writing “left brisker than
right” is more accurate than writing “nerve problem,” because the first statement is an observation and the second is a diagnosis. People who practice this
mindsetobserve first, interpret lateroften feel less anxiety and communicate better with clinicians if they do end up seeking care. And honestly, that’s the
best “real-world” benefit: the test becomes a way to understand your body’s signals without turning every signal into a scary story.






