
Table of Contents >> Show >> Hide
Note: This article is for educational purposes only and should not replace medical advice, diagnosis, or treatment from a licensed healthcare professional.
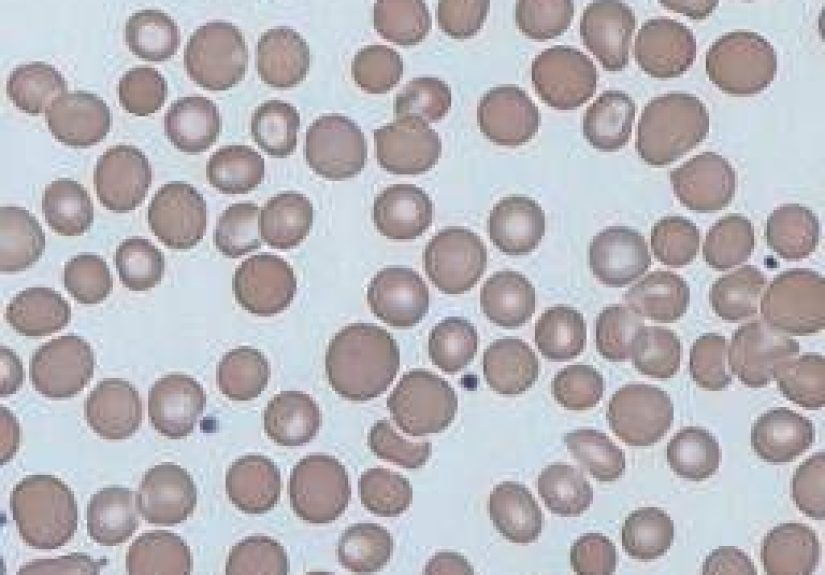
Anisocytosis sounds like the kind of word a tired medical student might accidentally invent after too much coffee, but it is a real and important blood-related finding. In simple English, anisocytosis means your red blood cells are not all the same size. Some may be smaller than normal, some larger, and some sitting awkwardly in the middle like they showed up to the wrong party.
Red blood cells have one superstar job: carrying oxygen from your lungs to the rest of your body. When these cells vary too much in size, it may signal that the body is struggling to make healthy blood cells. Anisocytosis is not usually a disease by itself. Instead, it is a clue, often seen on a complete blood count, that points doctors toward an underlying condition such as anemia, iron deficiency, vitamin B12 deficiency, folate deficiency, chronic disease, or certain inherited blood disorders.
The good news? Many causes of anisocytosis are treatable once the reason is identified. The less-good news? Guessing the cause based on symptoms alone is about as reliable as asking your refrigerator for financial advice. Blood tests matter. Context matters. A healthcare provider’s interpretation matters most.
What Is Anisocytosis?
Anisocytosis is a medical term used to describe red blood cells that vary noticeably in size. Healthy red blood cells are usually fairly uniform, round, flexible, and designed to move through blood vessels smoothly. When the size difference becomes significant, a lab may report anisocytosis on a blood smear or show an abnormal value called RDW, which stands for red cell distribution width.
RDW is part of many complete blood count reports. A high RDW generally means there is more variation in red blood cell size than expected. Doctors often interpret RDW together with other values, especially hemoglobin, hematocrit, MCV, MCH, and the appearance of cells under a microscope. One number alone rarely tells the whole story.
Anisocytosis vs. Poikilocytosis
Anisocytosis refers to differences in red blood cell size. Poikilocytosis refers to differences in red blood cell shape. Sometimes both happen together, which is called anisopoikilocytosis. That word may look like it lost a fight with a keyboard, but it simply means the red blood cells vary in both size and shape.
Common Causes of Anisocytosis
Anisocytosis can happen for several reasons. The most common causes are linked to anemia, a condition in which the body does not have enough healthy red blood cells or enough hemoglobin to carry oxygen efficiently.
1. Iron Deficiency Anemia
Iron deficiency anemia is one of the most common causes of anisocytosis. Iron is needed to make hemoglobin, the oxygen-carrying protein inside red blood cells. Without enough iron, red blood cells may become smaller than normal, a pattern known as microcytosis. As the body produces a mix of older normal-sized cells and newer smaller cells, RDW may rise and anisocytosis may appear.
Iron deficiency can result from heavy menstrual bleeding, pregnancy, low iron intake, digestive bleeding, ulcers, certain intestinal conditions, or poor absorption. In adults, especially when iron deficiency appears without an obvious explanation, doctors often look for hidden blood loss.
2. Vitamin B12 Deficiency
Vitamin B12 helps the body make DNA and healthy red blood cells. When B12 is low, red blood cells may become larger than normal, producing macrocytosis and anisocytosis. B12 deficiency may happen because of poor dietary intake, pernicious anemia, stomach surgery, intestinal disease, or trouble absorbing the vitamin.
B12 deficiency deserves attention because it can affect nerves as well as blood. Symptoms may include numbness, tingling, balance problems, memory issues, a sore tongue, weakness, or mood changes. In some people, nerve-related symptoms can occur even before anemia becomes obvious.
3. Folate Deficiency
Folate, also called vitamin B9, is another nutrient needed for normal red blood cell production. Low folate can lead to large, immature red blood cells and an abnormal blood picture. Folate deficiency may be related to poor diet, pregnancy, alcohol use, certain medications, or digestive conditions that affect absorption.
Folate is especially important during pregnancy because it supports fetal development. Pregnant people are commonly advised to get enough folic acid, but supplementation should still be discussed with a healthcare provider.
4. Mixed Nutritional Deficiencies
Sometimes anisocytosis is caused by more than one deficiency at the same time. For example, a person may have both iron deficiency and vitamin B12 deficiency. One problem can push red blood cells smaller, while the other pushes them larger. The result may be a confusing mix of cell sizes and lab values that require careful interpretation.
5. Thalassemia and Inherited Blood Disorders
Thalassemia is an inherited blood disorder that affects hemoglobin production. It may cause small red blood cells and anemia. Some people have mild forms and do not need major treatment, while others require ongoing specialist care. Sickle cell disease and other inherited blood disorders may also cause abnormal red blood cell production, destruction, or appearance.
6. Chronic Disease and Inflammation
Long-term inflammation, kidney disease, autoimmune conditions, infections, and some cancers can affect how the body uses iron and produces red blood cells. This is often called anemia of chronic disease or anemia of inflammation. In these cases, anisocytosis may appear alongside other abnormal blood test results.
7. Bone Marrow Conditions
The bone marrow is the factory where blood cells are made. If that factory has a quality-control problem, red blood cells may come out abnormal in size, number, or shape. Bone marrow disorders, including myelodysplastic syndromes, aplastic anemia, and certain cancers, can sometimes cause anisocytosis. These causes are less common but important, especially when blood counts are persistently abnormal.
8. Recent Blood Transfusion
After a blood transfusion, a person may temporarily have a mixture of their own red blood cells and donor red blood cells. Because these cells may differ in size, anisocytosis can show up for a while after transfusion.
Symptoms of Anisocytosis
Anisocytosis itself does not usually cause symptoms. The symptoms come from the underlying condition, most often anemia. Mild cases may be silent and discovered only during routine blood work. More noticeable cases can feel like your energy battery has been replaced with a potato.
Possible Symptoms Include:
- Fatigue or unusual weakness
- Shortness of breath, especially with activity
- Dizziness or lightheadedness
- Pale or yellowish skin
- Fast heartbeat or palpitations
- Cold hands and feet
- Headaches
- Chest discomfort in more serious cases
- Brittle nails or hair shedding with iron deficiency
- Numbness, tingling, or balance issues with vitamin B12 deficiency
Anyone with chest pain, fainting, severe shortness of breath, black or bloody stool, heavy uncontrolled bleeding, or extreme weakness should seek urgent medical care.
How Anisocytosis Is Diagnosed
Anisocytosis is usually detected through blood testing. A healthcare provider may start with a complete blood count, also called a CBC. This test measures several parts of the blood, including red blood cells, white blood cells, platelets, hemoglobin, hematocrit, MCV, and RDW.
Important Tests Doctors May Use
CBC: Shows whether anemia is present and provides red blood cell measurements.
RDW: Measures variation in red blood cell size. A high RDW can suggest anisocytosis.
MCV: Measures the average size of red blood cells. Low MCV may suggest microcytic anemia, often linked to iron deficiency. High MCV may suggest macrocytic anemia, often linked to vitamin B12 or folate deficiency.
Peripheral blood smear: Allows a lab professional to examine blood cells under a microscope. This can confirm size and shape changes.
Iron studies: Ferritin, serum iron, transferrin saturation, and total iron-binding capacity can help identify iron deficiency or inflammation-related anemia.
Vitamin B12 and folate tests: These help diagnose vitamin-related anemia.
Reticulocyte count: Reticulocytes are young red blood cells. This test helps show whether the bone marrow is responding properly.
Additional tests: Depending on the situation, doctors may check kidney function, liver function, thyroid levels, inflammatory markers, hemolysis labs, stool blood testing, or genetic testing.
Treatment for Anisocytosis
Treatment depends on the cause. Anisocytosis is a sign, not the final diagnosis. Treating the lab result without finding the reason is like mopping the floor while the sink is still overflowing. You may feel productive, but the real problem is still making a mess.
Treatment for Iron Deficiency
Iron deficiency treatment often includes oral iron supplements and dietary changes. Iron-rich foods include lean red meat, poultry, seafood, beans, lentils, spinach, tofu, pumpkin seeds, and iron-fortified cereals. Vitamin C foods such as citrus fruit, strawberries, tomatoes, and bell peppers can help the body absorb plant-based iron more effectively.
However, iron supplements should not be taken casually. Too much iron can be harmful, and iron deficiency may be caused by blood loss that needs medical evaluation. Some people need intravenous iron if they cannot absorb or tolerate oral iron, or if deficiency is severe.
Treatment for Vitamin B12 Deficiency
Vitamin B12 deficiency may be treated with oral supplements, high-dose therapy, or injections, depending on the cause and severity. People with absorption problems may need long-term treatment. Foods naturally rich in B12 include fish, meat, poultry, eggs, and dairy products. Some plant-based foods are fortified with B12, but people following vegan diets may need planned supplementation.
Treatment for Folate Deficiency
Folate deficiency is commonly treated with folic acid supplements and diet changes. Folate-rich foods include leafy greens, beans, peas, oranges, asparagus, avocado, and fortified grains. Doctors may check B12 status before or during folate treatment because folic acid can improve anemia while allowing B12-related nerve problems to continue unnoticed.
Treatment for Chronic Disease
When anisocytosis is linked to chronic disease, treatment focuses on managing the underlying condition. For example, kidney-related anemia may require kidney disease care and, in some cases, medications that support red blood cell production. Inflammatory or autoimmune conditions require targeted treatment from the appropriate specialist.
Treatment for Inherited Blood Disorders
Conditions such as thalassemia or sickle cell disease require individualized care. Treatment may include monitoring, folic acid, transfusions, iron management, medications, or specialist-directed therapies. These conditions should be managed with a hematologist when possible.
Can Anisocytosis Be Prevented?
Not every case can be prevented, especially when genetics, chronic disease, or bone marrow disorders are involved. Still, some causes can be reduced with practical habits. Eating a balanced diet with enough iron, vitamin B12, and folate helps support normal red blood cell production. Managing heavy menstrual bleeding, digestive symptoms, chronic conditions, and medication side effects can also lower risk.
Routine checkups matter, especially for people who are pregnant, have heavy periods, follow restrictive diets, have digestive disorders, have kidney disease, or have a history of anemia. Blood work can catch problems before symptoms become dramatic.
When Should You See a Doctor?
You should talk with a healthcare provider if a lab report mentions anisocytosis, high RDW, anemia, low hemoglobin, abnormal MCV, or unusual red blood cell findings. You should also seek care if you have persistent fatigue, shortness of breath, dizziness, palpitations, pale skin, numbness, tingling, or unexplained weakness.
Do not try to diagnose the cause based only on internet research. The internet is excellent for learning and occasionally for finding recipes that use suspicious amounts of cheese. It is not a substitute for blood tests, medical history, and professional interpretation.
Living With Anisocytosis: Practical Experience and Everyday Lessons
People often discover anisocytosis by accident. They go in for a routine physical, a school sports form, a pregnancy visit, a pre-surgery check, or a “why am I so tired?” appointment, and the lab report comes back with terms that sound more alarming than they may actually be. Seeing words like “anisocytosis present” can be unsettling. Many patients immediately wonder whether something serious is happening. The honest answer is: sometimes it is simple, sometimes it needs more testing, and guessing rarely helps.
One common experience is the slow creep of iron deficiency. A person may feel tired for months and blame school, work, parenting, poor sleep, stress, or the heroic decision to survive on coffee and crackers. Then stairs start feeling harder. Workouts feel oddly dramatic. Standing up too fast brings dizziness. A blood test finally shows anemia, high RDW, and red blood cells that are smaller than expected. In that situation, anisocytosis becomes the clue that helps point toward iron deficiency. Treatment may involve iron supplementation, dietary changes, and, importantly, finding out why iron is low in the first place.
Another experience is vitamin B12 deficiency. This can be sneakier because symptoms may involve both energy and nerves. Someone might notice fatigue, brain fog, tingling feet, clumsy balance, or a sore tongue. They may assume they are just “getting older” or sitting too long at a computer. Blood work may show larger red blood cells and anisocytosis. Once B12 deficiency is identified, treatment can make a major difference, but timing matters because nerve symptoms should not be ignored.
For pregnant people, anisocytosis may appear during routine prenatal testing. Pregnancy increases the need for iron and folate, so mild abnormalities are not rare. Still, they deserve follow-up. Good prenatal care helps protect both the pregnant person and the developing baby. This is not the moment to freestyle supplements like a kitchen chemist. Proper dosing and testing matter.
For people with chronic illnesses, anisocytosis can feel like one more confusing number in a lab report full of confusing numbers. Kidney disease, inflammatory conditions, liver disease, thyroid problems, and autoimmune disorders can all affect blood production. In those cases, the most helpful approach is usually steady follow-up, tracking trends over time, and treating the root condition rather than chasing one lab value.
The biggest lesson from real-world experience is that anisocytosis should be treated as a clue, not a verdict. A lab report is a map, not the destination. The right next step is usually a calm conversation with a healthcare provider, a review of symptoms, and targeted testing. Many people improve once the cause is found and treated. The key is not to panic, not to ignore it, and definitely not to self-prescribe random supplements from the internet’s glowing carnival of miracle claims.
Conclusion
Anisocytosis means red blood cells vary more in size than expected. It is most often connected to anemia and may be caused by iron deficiency, vitamin B12 deficiency, folate deficiency, chronic inflammation, inherited blood disorders, bone marrow conditions, or recent transfusion. Symptoms, when present, usually come from the underlying cause and may include fatigue, shortness of breath, dizziness, pale skin, palpitations, or nerve-related changes.
The best treatment depends on the diagnosis. Iron deficiency may require iron replacement and investigation for blood loss. Vitamin deficiencies may require supplements and diet changes. Chronic disease or inherited conditions need individualized medical care. With the right testing and treatment plan, anisocytosis often becomes less mysterious and much more manageable.




