
Table of Contents >> Show >> Hide
- What Is Breast Tomosynthesis, Exactly?
- DBT vs 2D Mammography: What’s the Practical Difference?
- Who Might Benefit Most from Breast Tomosynthesis?
- What to Expect During a DBT Appointment
- Does DBT Actually Improve Accuracy?
- Radiation Dose: Should You Worry?
- Screening Guidelines: Where Does DBT Fit In?
- Cost and Insurance: The Awkward but Necessary Conversation
- How Radiologists Read DBT (And Why It Can Reduce Callbacks)
- Research Still in Progress: What We’re Learning Next
- Questions to Ask Before You Book
- Bottom Line
- Experiences with Breast Tomosynthesis: What People Actually Notice (500+ Words)
Breast tomosynthesisalso called digital breast tomosynthesis (DBT) or the more marketable nickname
“3D mammography”is basically mammography’s glow-up. Instead of taking just a couple flat pictures
of the breast, DBT captures multiple low-dose X-ray images from different angles and reconstructs them into thin
“slices” you can scroll through. Think: flipping through pages of a book instead of judging the whole plot from the cover.
If you’ve ever heard someone say, “My mammogram was fine… until I got called back,” you already know why DBT matters.
Overlapping tissue in a standard 2D mammogram can hide a real findingor create a fake one. DBT is designed to reduce
that “is it something or just a tissue pile-up?” problem, especially for people with dense breasts.
What Is Breast Tomosynthesis, Exactly?
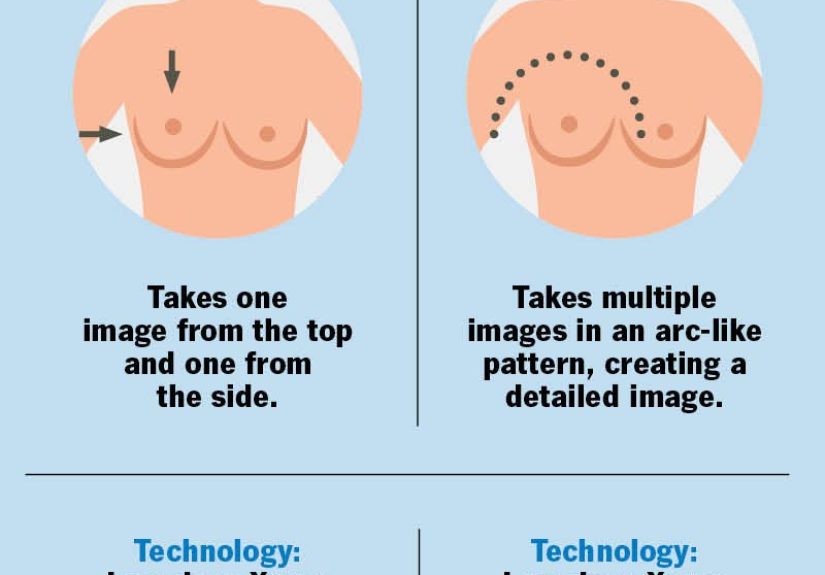
During a DBT exam, your breast is positioned and gently (okay, sometimes not-so-gently) compressedjust like a standard
mammogram. The difference is the X-ray tube moves in a small arc over the breast, capturing a series of images from
multiple angles. A computer then reconstructs these into a 3D-like set of thin images that radiologists review slice by slice.
Why the “Slices” Matter
In 2D mammography, everything in the breast gets projected into a single image per view, like layering every sheet of
lasagna into one photo and trying to count noodles. DBT reduces the impact of tissue overlap, which can make it easier
to see masses, architectural distortion, or asymmetriesand easier to decide when something is truly suspicious versus
just normal tissue playing tricks.
DBT vs 2D Mammography: What’s the Practical Difference?
Most screening protocols today use DBT alongside either a traditional 2D mammogram or a synthetic 2D image
generated from the DBT data. The synthetic 2D approach exists for a very human reason: we like better information, but we
also like not increasing radiation more than necessary.
- 2D mammography: Two main views per breast, flat images, excellent screening tool but can be limited by overlap.
- DBT (3D mammography): Multiple angled images reconstructed into thin slices to reduce overlap.
- Synthetic 2D: A 2D-like image created from the DBT dataset, often used to avoid taking separate 2D exposures.
Who Might Benefit Most from Breast Tomosynthesis?
DBT can be used for both screening (routine checks when you don’t have symptoms) and
diagnostic imaging (when there’s a lump, pain, nipple discharge, a previous abnormal result, or other concerns).
Many facilities now offer DBT as their standard screening option, while others offer it selectively.
Dense Breasts: The “Crowded Closet” Problem
Breast density refers to the proportion of fibrous and glandular tissue compared to fatty tissue on a mammogram.
Dense tissue can make cancers harder to see on 2D images because both dense tissue and many abnormalities appear white.
DBT’s slice-by-slice view can help untangle that visual overlap and has been shown in many studies to improve detection
and reduce false alarms in people with dense breasts.
If You’ve Been Called Back Before
Being recalled after a screening mammogram is common and often turns out to be nothing seriousbut it’s stressful,
inconvenient, and can lead to extra imaging. One of the most consistent findings in DBT research is a reduction in
recall rates (fewer “come back for more pictures” calls), particularly in U.S. screening settings where baseline recall
rates have historically been higher.
What to Expect During a DBT Appointment
The overall experience is very similar to a standard mammogram, with a few small differences. Most exams take roughly
the same amount of time from start to finish (often around 10–15 minutes, with actual imaging much quicker).
Step-by-Step (No Dramatic Plot Twists)
- Prep: You’ll typically be asked not to wear deodorant, powders, or lotions on the chest/underarm area (they can mimic calcifications).
- Positioning: A technologist positions the breast on the plate.
- Compression: The breast is compressed briefly to spread tissue and reduce motion blur.
- Image capture: The tube moves in a small arc to capture multiple images. You may be asked to hold your breath for a moment.
- Repeat views: Usually two standard views per breast for screening; diagnostic imaging may include extra views.
The compression is often the part people worry about most. The honest truth: it can be uncomfortable. The helpful truth:
it’s brief, and it improves image quality while potentially lowering the need for repeat imaging.
Does DBT Actually Improve Accuracy?
Broadly speaking, evidence shows DBT can improve key screening performance metrics compared with 2D mammography alone:
higher cancer detection rates in many settings and fewer false positives/recalls. Large U.S. observational studies and
systematic reviews have reported improvements, although the size of the benefit can vary by population, breast density,
screening interval (annual vs biennial), and facility practices.
Fewer False Positives and Recalls (Often a Big Deal)
False positives are abnormal screening results that ultimately do not turn out to be cancer. They can lead to more imaging,
biopsies, anxiety, and a week of you staring at your phone like it owes you money. Many studies have found DBT lowers recall
rates and can modestly reduce false positives over time.
More Cancers Found (Especially When Tissue Overlaps)
DBT’s slice viewing can reveal cancers that might be obscured on 2D images, particularly in dense tissue. That said, no test
is perfect: DBT is a powerful tool, not a magical “never miss anything” spell.
Radiation Dose: Should You Worry?
Mammography uses low-dose X-rays, and DBT is designed to stay within established safety standards. Radiation dose
discussions often come down to what protocol is used:
- DBT + separate 2D mammography can be higher than 2D alone.
- DBT + synthetic 2D can reduce exposure compared with doing both DBT and separate 2D images.
In practical terms, imaging systems and protocols are regulated and monitored, and facilities must meet quality and safety
requirements. If radiation is a concern for you (very reasonable!), ask your imaging center whether they use synthetic 2D images
with DBT and what their typical protocol is.
Screening Guidelines: Where Does DBT Fit In?
DBT is considered an effective screening modality alongside standard digital mammography. Major guideline groups differ on
exact ages and intervals (because medicine loves nuance), but here’s a simple way to think about it:
A Practical Framework
- Average risk: Follow evidence-based screening guidance, and consider DBT if availableespecially if you have dense breasts or prior recalls.
- Higher than average risk: Family history, genetic mutations, prior chest radiation, or certain syndromes may require earlier and/or supplemental screening plans.
- Dense breasts: DBT may help, but additional screening (like ultrasound or MRI) is a more individualized decisionan active area of research.
Importantly, DBT does not replace clinical judgment. If you have symptoms (new lump, nipple discharge, skin changes),
don’t wait for your next screeningseek medical evaluation.
Cost and Insurance: The Awkward but Necessary Conversation
DBT often costs more than 2D mammography, and coverage can vary by insurer and state. The trend in the U.S. has been toward
broader coverage, but it’s not universal. Before your appointment, ask:
- Is DBT billed differently than 2D mammography?
- Will I have an out-of-pocket cost?
- Do you use DBT with synthetic 2D, or do you also take separate 2D images?
It’s not fun to make healthcare decisions with a calculator in one hand and an insurance portal in the other, but here we are.
The good news: most imaging centers are used to these questions and can help you estimate costs.
How Radiologists Read DBT (And Why It Can Reduce Callbacks)
With DBT, radiologists scroll through thin image slices to evaluate structures at different depths. This can make it easier
to decide whether a questionable area is a real mass or simply overlapping tissue. In diagnostic settings, DBT can also help
localize findings more precisely for follow-up imaging or biopsy planning.
A Concrete Example
Imagine a routine screening shows a vague shadow in the upper outer breast on a 2D image. In DBT slices, that “shadow”
may separate into normal tissue layersno mass, no distortion, no problemmeaning fewer unnecessary callbacks. On the other
hand, if the shadow persists across slices with suspicious features, DBT can help confirm that it’s not just overlap and guide
the next steps.
Research Still in Progress: What We’re Learning Next
DBT has strong evidence for improving detection and reducing recalls, but researchers are still working on longer-term outcomes,
including how DBT affects the rates of advanced cancers and how it performs across diverse populations and screening intervals.
Large studies comparing 2D to DBT are ongoing to clarify these outcomes even further.
Questions to Ask Before You Book
- Do you offer DBT (3D mammography) for screening and diagnostic exams?
- Do you create synthetic 2D images from the DBT dataset?
- How and when will I receive results?
- If I’m called back, what does the follow-up process look like?
- Do you have dedicated breast imaging radiologists?
Bottom Line
Breast tomosynthesis is a major upgrade in how we image breast tissue: more angles, less overlap, andoftenfewer stressful
callbacks. It’s not a replacement for good screening habits or individualized risk discussions, but it is a powerful tool that
many U.S. centers now use routinely. If DBT is available to you, it’s worth consideringespecially if you have dense breasts,
prior recalls, or you simply want the clearest picture modern mammography can provide.
And yes: the compression part still exists. But at least now the images are working harder than your anxiety.
Experiences with Breast Tomosynthesis: What People Actually Notice (500+ Words)
Let’s talk about the part brochures rarely capture: the lived experience of walking into a breast imaging center, putting on
the open-front gown (a fashion statement no one asked for), and trying to act casual while your brain runs a full-length
documentary titled “Every Bad Thing That Could Happen”.
First-timers often say the biggest surprise is how normal the appointment feels. The room is usually calm,
the technologist is all business (in a reassuring way), and the actual image capture is quick. People who choose DBT expecting
a dramatically different process from 2D mammography tend to leave thinking, “Wait… that was it?” The machine looks similar,
the positioning is similar, and the compression is still the headline act. The difference is subtle: during DBT, some notice
the X-ray tube moving in a small arc. It’s not a wild sci-fi swoopit’s more like a polite nod from the machine.
People with dense breasts often describe DBT as a “confidence upgrade,” not because they can feel the technology
doing anything special, but because they’ve heard (or experienced) the cycle of callbacks that can happen with 2D images. For
some, the most meaningful “experience” is what doesn’t happen afterward: fewer frantic calls, fewer “we just need a couple
extra images,” fewer days spent trying to decode radiology scheduling into emotional certainty. Not everyone avoids a callbackDBT
isn’t a get-out-of-follow-up-free cardbut many patients feel reassured knowing the radiologist can review the breast in thin slices.
People who’ve had a prior callback often arrive with a very specific kind of tension: not fear of the exam itself,
but fear of the aftermath. These patients tend to appreciate clear communication: “When will I get results?” “Will you call me
either way?” “If something looks questionable, what’s the next step?” In that context, DBT can feel like a practical way to reduce
uncertainty. The mental shift is less “I’m doing this to find something” and more “I’m doing this to get a clearer answer.”
From the technologist’s side (as many patients recount after chatting during positioning), the experience is often about
precision and comfort at the same time. Positioning matterstiny adjustments can affect image qualityand techs typically coach
breathing and posture to reduce motion blur. Patients frequently say that a calm, confident technologist makes the exam dramatically
easier. The best ones narrate just enough: what they’re doing, what you’ll feel, and how long it will last. That predictability is
underrated medicine.
From the radiologist’s side (as explained in patient-friendly summaries), DBT reading is often described like “scrolling
through layers.” Patients who hear this explanation tend to feel relief: it’s easier to trust a result when you understand the
method. When someone is told, “We can separate overlapping tissue,” it reframes the whole process. The exam isn’t just a snapshot;
it’s a series of views designed to reduce visual confusion.
Finally, there’s a very real emotional experience that shows up across many stories: the appointment becomes easier the second time.
Whether you do DBT or 2D, familiarity helps. People learn what to wear, how to schedule around their menstrual cycle if they’re prone to
tenderness, and how to ask for a moment if positioning feels uncomfortable. DBT doesn’t erase the human feelings around screeningbut for
many, it makes the results feel a little more grounded, a little less like guesswork, and a little more like an informed next step.





