Table of Contents >> Show >> Hide
- Table of Contents
- What diabetic retinopathy is (and why your retina cares)
- Why these eye changes happen
- Early retinal changes: what doctors see before you feel anything
- Nonproliferative diabetic retinopathy (NPDR): mild → severe
- Diabetic macular edema (DME): when “central vision HQ” gets flooded
- Proliferative diabetic retinopathy (PDR): new vessels, new problems
- How eye doctors spot these changes
- Treatment: how we protect vision
- How to lower your risk and slow progression
- When symptoms are urgent
- Conclusion
- Real-world experiences: what people commonly notice and feel (and what the process is like)
Friendly heads-up: This article is for general education, not personal medical advice. If you have diabetes and any vision changesespecially sudden onescontact an eye care professional promptly.
What diabetic retinopathy is (and why your retina cares)
Your retina is the thin, light-sensing layer lining the back of your eye. Think of it like the sensor in a phone camera: it turns light into signals your brain understands. Diabetic retinopathy happens when diabetes damages the tiny blood vessels that feed that “camera sensor.” Those vessels can weaken, leak, close off, orlatergrow abnormal new branches that cause bleeding and scarring.
Here’s the tricky part: diabetic retinopathy can be busy changing your retina long before your vision starts complaining. That’s why regular dilated eye exams matter even when you feel fine. In the early stages, many people have no symptoms, but the retina is already collecting clues that a trained eye doctor can see.
Why these eye changes happen
High blood sugar over time can damage blood vessels throughout the body, including the retina’s delicate capillary network. When these tiny vessels get stressed, several things can happen:
- Vessel walls weaken → they bulge (microaneurysms) and leak fluid or blood.
- Leakage → swelling in retinal tissue and deposits of fats/proteins (exudates).
- Blockage/poor flow → parts of the retina don’t get enough oxygen (ischemia).
- Oxygen shortage → the eye releases signals (like VEGF) that encourage new vessel growthunfortunately, these new vessels are fragile troublemakers.
Risk generally increases with longer duration of diabetes, higher average blood sugar, and other factors such as high blood pressure and abnormal cholesterol. If you want the retina to stay calm, your overall metabolic “weather forecast” matters.
Early retinal changes: what doctors see before you feel anything
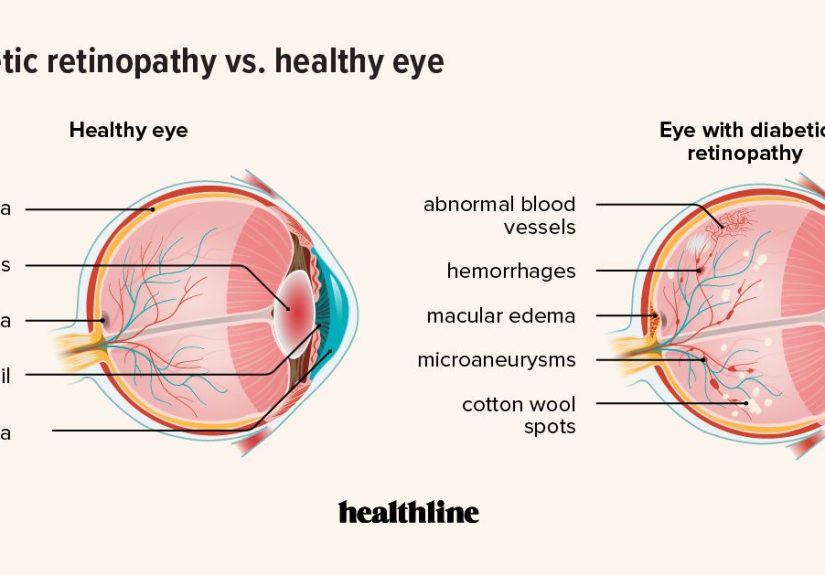
Diabetic retinopathy often starts like a mystery novel: the important plot points appear in the background first. During a dilated exam or retinal imaging, an eye doctor may see:
Microaneurysms (tiny bulges in capillaries)
These are among the earliest visible signs. They’re like little weak spots in vessel walls that can leak. Alone, they may not change your vision, but they’re a signal that the retinal vessels are under stress.
Retinal hemorrhages (small bleeds)
When stressed vessels leak blood, it can show up as pinpoint or blot-like spots in the retina. The presence and amount help doctors grade severity.
Hard exudates (fatty deposits)
When fluid leaks, the watery part can be reabsorbed, but leftover lipids can remain as yellowish deposits. Sometimes they form rings around leaking microaneurysmslike the retina is highlighting the “leaky faucet.”
Cotton-wool spots (soft exudates)
These look like small fluffy white patches and are linked to areas where nerve fibers didn’t get enough oxygenthink of them as “retinal traffic jams” caused by poor blood flow.
Important note: seeing these changes doesn’t automatically mean you’ll lose vision tomorrow. It does mean the retina has started keeping receiptsand your eye doctor knows how to read them.
Nonproliferative diabetic retinopathy (NPDR): mild → severe
Most diabetic retinopathy begins as nonproliferative, meaning there are vessel changes and leakage, but no abnormal new vessel growth yet. NPDR is commonly described in a spectrum:
Mild NPDR
Often includes microaneurysms and a few small hemorrhages. Many people have no symptoms. This stage is frequently a wake-up call to tighten overall diabetes management and keep up with monitoring.
Moderate NPDR
More bleeding spots, more leakage, and sometimes early signs that blood flow is being compromised. Vision may still be normal unless the macula becomes involved (more on that next).
Severe NPDR
This stage suggests widespread vessel damage and significant areas of reduced blood flow. The retina, feeling under-supplied, is more likely to send strong signals that can trigger abnormal vessel growth. In other words: severe NPDR is the retina standing on the balcony yelling, “We need oxygen down here!”
Across NPDR stages, symptoms can range from none to mild blurrinessespecially if swelling affects the macula. A person may notice vision fluctuates day to day, particularly when blood sugar levels vary.
Diabetic macular edema (DME): when “central vision HQ” gets flooded
The macula is the small central area of the retina responsible for sharp, straight-ahead visionreading, driving, recognizing faces, and spotting your friend across the cafeteria. (Or your phone at 1% battery across the room. Very important survival skill.)
Diabetic macular edema happens when leaky vessels cause fluid buildup in or near the macula. This can lead to:
- Blurry central vision (like someone smudged the center of your glasses)
- Wavy or distorted lines (straight edges may look bent)
- Trouble reading or seeing fine detail
- Colors looking “off” or less vivid
DME can occur at different stages of diabetic retinopathy. It’s also one of the most common reasons diabetic retinopathy starts affecting vision in a noticeable way. Eye doctors often use OCT imaging to measure and track macular swelling over time.
Proliferative diabetic retinopathy (PDR): new vessels, new problems
When the retina is starved for oxygen long enough, it may grow new blood vesselsa process called neovascularization. Sounds helpful, right? New vessels! Fresh supply routes!
Unfortunately, these new vessels are usually fragile, disorganized, and prone to bleeding. That’s when NPDR can progress to proliferative diabetic retinopathy (PDR), which carries a higher risk of major vision loss if untreated.
Vitreous hemorrhage (bleeding into the eye’s gel)
The eye is filled with a jelly-like substance called the vitreous. If new vessels bleed, blood can cloud that gel. People may notice:
- Sudden new floaters (dots, strands, cobwebs)
- A hazy curtain or “smoke” in vision
- Sudden drop in vision clarity
Scar tissue and traction retinal detachment
Abnormal vessels can be accompanied by scar tissue. As scar tissue contracts, it can tug on the retina. In severe cases, that pulling can lift the retina away from the back of the eye (traction retinal detachment). This is a medical emergency risk because the retina can’t do its job if it’s not where it belongs.
Neovascular glaucoma (pressure trouble)
In some cases, new vessels can grow in areas that interfere with normal fluid drainage in the eye, raising pressure and damaging the optic nerve. This is less common than DME but serious.
The big takeaway: PDR is not the time to “wait and see.” It’s the time to “see and treat.”
How eye doctors spot these changes
Eye care pros have a toolkit designed specifically for catching diabetic retinopathy before it catches you. Common methods include:
Dilated eye exam
Drops widen the pupil so the doctor can examine the retina and optic nerve. This is often the front door to detection: microaneurysms, hemorrhages, exudates, and new vessel growth can be identified during a comprehensive exam.
Retinal photography (fundus photos)
High-resolution photos document the retina over time. This helps track progression and supports tele-retina screening programs in some settings.
Optical coherence tomography (OCT)
OCT is like an ultrasound, but with light. It creates cross-sectional images of the retina and is especially useful for diagnosing and monitoring macular edema.
Fluorescein angiography
A dye is injected into the bloodstream, and a special camera captures how it flows through retinal vessels. This can show leakage, blocked areas, and abnormal new vesselsbasically, a “traffic report” for retinal circulation.
Treatment: how we protect vision
Treatment depends on the stage and which changes are present. Some people need careful monitoring; others need active therapy to reduce swelling, stop bleeding, or prevent further damage.
1) Systemic control: the foundation that affects your eyes
Even the best eye treatment can’t fully outvote uncontrolled diabetes. Improving average blood sugar, managing blood pressure, and addressing cholesterol are strongly linked with lowering risk of progression. In plain English: the retina likes steady, stable conditionsnot sugar roller coasters and pressure spikes.
2) Anti-VEGF injections
VEGF is one of the chemical signals that encourages leaky vessels and abnormal new vessel growth. Anti-VEGF medicines injected into the eye can reduce macular swelling (DME) and help treat PDR. Many people hear “injection in the eye” and immediately try to teleport out of the roomunderstandablebut these procedures are typically done with numbing medicine, and many patients describe more pressure than pain.
3) Corticosteroid treatment (selected cases)
Steroids can reduce inflammation and swelling in certain situations, including some cases of DME. They may be delivered by injection or implant. Because steroids can raise eye pressure or speed cataract formation in some people, doctors weigh benefits and risks carefully.
4) Laser treatment
Laser therapy can be used in different ways:
- Focal/grid laser (less common than it used to be for DME, but still used in selected situations)
- Panretinal photocoagulation (PRP) for PDR to reduce the retina’s oxygen demand and help regress abnormal new vessels
Laser treatment isn’t about “burning away your vision.” It’s about preventing severe vision loss by targeting problematic areas and reducing signals that drive harmful vessel growth.
5) Vitrectomy surgery
If there’s persistent vitreous hemorrhage (blood clouding the eye) or traction pulling on the retina, a retina specialist may recommend vitrectomy. This procedure removes the vitreous gel (and blood within it) and can address scar tissue that threatens the retina.
Many treatment plans combine approaches: for example, anti-VEGF plus laser for PDR, or anti-VEGF as primary therapy for DME with close imaging follow-up.
How to lower your risk and slow progression
Not every case of diabetic retinopathy can be prevented, but a lot of damage can be delayedor kept milderby consistent habits and follow-up care:
- Get routine dilated eye exams on the schedule your clinician recommends. Early disease can be silent.
- Keep blood sugar in target range as often as possible. Long-term control matters more than occasional perfect days.
- Manage blood pressure. High pressure adds stress to delicate retinal vessels.
- Address cholesterol/lipids, which may relate to exudates and vascular health.
- Don’t skip follow-ups if your doctor wants more frequent monitoringthose intervals are based on real risk.
- Tell your care team about pregnancy plans if you have preexisting diabetes, because retinopathy can worsen during pregnancy and may need closer monitoring.
If you’re someone who loves checklists, here’s a retina-friendly mantra: screen, steady, and show up. Screen (eye exams), keep things steady (glucose/BP/lipids), and show up (follow-up visits and treatment if needed).
When symptoms are urgent
Some symptoms deserve same-day or urgent evaluation, especially for people with diabetes:
- Sudden shower of floaters or new cobweb-like strands
- A dark curtain or shadow moving across vision
- Sudden major vision loss in one or both eyes
- Eye pain with redness and blurred vision (especially with nausea), which can suggest pressure problems
These can be signs of vitreous hemorrhage, retinal detachment, or other serious issues. “Wait and see” is great for movie sequelsnot for sudden eye symptoms.
Conclusion
Diabetic retinopathy changes the eye in a recognizable pattern: early vessel weakening and leakage (microaneurysms, hemorrhages, exudates), swelling that can blur central vision (macular edema), andif oxygen shortage becomes severeabnormal new vessel growth that can bleed and scar (proliferative disease). The surprising part is how often these changes begin quietly.
The good news is that modern screening and treatmentsespecially retinal imaging, anti-VEGF therapy, laser approaches, and surgery when neededcan significantly reduce the risk of severe vision loss when problems are caught early and followed closely. Pair that with steady diabetes management, and your retina has a much better chance of staying the reliable “camera sensor” you deserve.
Real-world experiences: what people commonly notice and feel (and what the process is like)
Medical descriptions are helpful, but they can feel like reading a car manual when what you really want to know is: “What does this actually look like in day-to-day life?” Here are experiences many people report when diabetic retinopathy or diabetic macular edema starts affecting visionand what the care journey often feels like.
“My vision isn’t exactly blurry… it’s just not dependable.”
A common early complaint isn’t total blurit’s inconsistency. Some people say their vision is crisp in the morning and foggy later, or it changes with blood sugar swings. Others notice they’re suddenly adjusting screen brightness, squinting at street signs they used to read easily, or needing more light to see fine print. This can happen when the macula is slightly swollen or when the eye’s focusing system is affected by glucose changes.
Floaters: the “snow globe” moment
Many people have a few harmless floaters, but those with proliferative changes sometimes describe a sudden “snow globe” effectdark specks, strings, or cobwebs appearing quickly. It can be scary because it feels like something is physically in the eye (and, in a way, it is: blood or debris in the vitreous). People often say the biggest surprise is how fast it happensnormal-ish vision, then suddenly a haze.
Reading and faces get weirdly harder
When diabetic macular edema is involved, people often report that small text becomes tiring. Lines may look slightly wavy, or words seem to fade in and out. Recognizing faces at a distance can feel more difficultnot because everything is dark, but because detail has gone missing. Some describe it like watching a video that keeps buffering right at the important parts.
The dilated exam: bright lights, blurry selfies
If you’ve never had a dilated exam, here’s the honest version: the drops can sting a little, the lights are bright, and your near vision will likely be blurry for a few hours. Many people plan the visit around work or school because screens and reading can be annoying afterward. Sunglasses help, and yesyour post-exam selfie may look like you’ve just seen a ghost with very strong opinions about fluorescence.
OCT imaging: fast, painless, surprisingly cool
OCT is usually quick and noninvasive. People often say it feels like taking a high-tech photo while staring at a fixation target. The neat part is that doctors can show you a cross-section of your retinasome patients find it reassuring to see swelling go down over time, because it turns treatment from “I hope it’s working” into “Oh, that bump is literally smaller.”
Intravitreal injections: fear first, then routine
The idea of an eye injection is a top-tier nightmare for many humans. In practice, people often report that the anticipation is worse than the procedure. Clinics use numbing drops (and other steps to reduce discomfort and infection risk). Patients commonly describe pressure, a brief scratchy sensation afterward, and a gritty feeling for a day. Most also say that once they realize it’s quick and controlled, the fear drops dramaticallythough nobody is campaigning to make it a hobby.
Living with follow-ups
One of the biggest “real” challenges is not a single test or treatmentit’s the rhythm of care: repeat visits, imaging, and tracking changes over time. People who do well often build a simple system: calendar reminders, asking for written visit summaries, and pairing eye appointments with other diabetes check-ins. Many also find that protecting vision becomes a powerful motivation to keep glucose and blood pressure steadiernot perfect, just steadier.
If you’re dealing with diabetic retinopathy, it can help to remember: you’re not failing because you need monitoring or treatment. You’re doing what modern medicine is designed forcatching changes early and protecting your future vision.






